Mechanical Circulatory Support: Understanding Advanced Heart Support Devices
Table of Contents
- Introduction
- What Is Mechanical Circulatory Support?
- When Is Mechanical Circulatory Support Used?
- Temporary Versus Durable Mechanical Circulatory Support
- Types of Mechanical Circulatory Support Devices
- Decision Support: "Bridge" and "Destination Therapy"
- What Are the Risks of Mechanical Circulatory Support?
- Who May Not Be Suitable for Mechanical Support?
- Myth vs. Fact: Mechanical Circulatory Support
- Actionable Checklist: What to Ask the Heart Team
- Advanced Cardiac Evaluation at CANES Clinic
- FAQs
Book a Consultation
Prevention is better than cure. Talk to our specialists today.
When the heart becomes too weak to pump enough blood to the brain, kidneys, and other vital organs, medicines alone may not provide sufficient support. In selected patients, doctors may use mechanical circulatory support (commonly called MCS) to temporarily or permanently assist the heart’s pumping function.
Mechanical circulatory support is not a single treatment. It includes several specialized devices ranging from a temporary intra-aortic balloon pump to a permanently implanted left ventricular assist device (LVAD). Some devices support only one side of the heart, while others support both the heart and lungs simultaneously. The right device depends entirely on the cause and severity of your heart failure, how quickly support is required, whether natural recovery is expected, and whether the patient may be eligible for a future heart transplant.
At CANES Cardio & Neuro Clinic, a specialized cardiovascular care centre in Hyderabad, patient education and individualized cardiac assessment are central to our treatment process. Guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist specializing in complex cardiology, our approach emphasizes careful evaluation, shared decision-making, and the appropriate coordination of advanced cardiac care.
Quick Answer
Mechanical circulatory support refers to advanced medical devices that help the heart circulate blood when it cannot pump effectively on its own. Temporary devices such as an intra-aortic balloon pump, percutaneous ventricular assist device, or VA-ECMO may be used during cardiogenic shock or recovery from heart surgery. Durable devices such as an LVAD may support a patient for months or years while awaiting transplantation or as long-term treatment when transplantation is not suitable.
Mechanical Circulatory Support at a Glance
Device | What It Supports | Typical Role |
|---|---|---|
Intra-aortic balloon pump (IABP) | Assists the left heart indirectly | Short-term stabilization and reduction of cardiac workload. |
Percutaneous VAD | Left or right ventricle, depending on the device | Temporary support during severe heart failure, cardiogenic shock, or high-risk procedures. |
VA-ECMO | Heart and lungs | Emergency support for profound cardiac or cardiopulmonary failure. |
LVAD / RVAD | Left ventricle / Right ventricle | Bridge to transplantation, bridge to recovery, or long-term destination therapy. |
BIVAD | Both ventricles | Support when both sides of the heart are failing simultaneously. |
Total Artificial Heart | Replaces both native ventricles and valves | Primarily a bridge to heart transplantation. |
What Is Mechanical Circulatory Support?
Mechanical circulatory support is the use of a highly specialized mechanical device to improve blood flow and deliver oxygen to vital organs when the natural heart cannot maintain adequate circulation.
Key Takeaway: MCS supports the circulation to keep you alive, but it does not necessarily cure the underlying disease that caused the heart to fail; medical treatment must continue alongside the device.
Detailed Explanation
Current cardiology guidelines emphasize matching the specific device to the patient’s exact form of cardiac failure rather than using the same device for every patient with low blood pressure. Depending on the device chosen, mechanical circulatory support may:
Reduce the heavy workload placed on a failing ventricle.
Increase the amount of oxygenated blood reaching the brain and kidneys.
Support circulation while the native heart rests and recovers.
Maintain the patient while doctors determine the safest next treatment step.
Provide continuous support while the patient waits for a donor heart.
Serve as a permanent, long-term therapy when a transplant is not an option.
When Is Mechanical Circulatory Support Used?
Mechanical circulatory support is utilized when the heart cannot deliver enough oxygenated blood to the body despite appropriate medicines, typically during cardiogenic shock, advanced heart failure, or recovery from complex cardiac surgery.
Key Takeaway: These devices are deployed in life-threatening scenarios where the heart requires immediate, powerful mechanical assistance to prevent irreversible damage to other vital organs.
Detailed Explanation
Common clinical situations requiring MCS include:
Cardiogenic Shock: This occurs when severe cardiac dysfunction prevents sufficient blood from reaching the brain and organs. It is a life-threatening emergency. Temporary mechanical support is considered when blood pressure remains dangerously low despite medicines or emergency angioplasty.
Advanced Heart Failure: Patients may experience severe breathlessness, fatigue, and organ dysfunction despite optimal guideline-directed medical therapy (GDMT). A durable LVAD may be considered when the left ventricle can no longer maintain circulation.
Recovery After Cardiac Surgery: Temporary support may help a heart that has difficulty resuming effective pumping after complex open-heart surgery, providing time to heal.
Severe Heart Attack: A major heart attack may damage enough muscle to cause cardiogenic shock. While the blocked artery must be fixed, the device supports circulation while the muscle recovers.
Myocarditis or Sudden Cardiomyopathy: Severe inflammation can cause sudden heart failure. Temporary MCS provides critical time for the heart to rest while the inflammation is treated.
Waiting for Heart Transplantation: Devices like an LVAD, BIVAD, or total artificial heart maintain circulation while an eligible patient waits for a suitable donor heart.
Temporary Versus Durable Mechanical Circulatory Support
Temporary MCS devices are used for hours or weeks to stabilize a patient in an intensive care setting, while durable MCS devices are surgically implanted to provide long-term support for months or years.
Key Takeaway: The choice between temporary and durable support depends entirely on whether the heart is expected to recover quickly or if permanent mechanical assistance is required.
Detailed Explanation
Temporary MCS These devices are generally inserted through blood vessels in the catheterization lab or through a limited surgical approach. They are used when the condition may be reversible, immediate stabilization is required, or doctors need time to assess neurological recovery before making a long-term plan.
Durable MCS Durable devices (like an LVAD) are surgically implanted into the chest for longer-term support. Patients being considered for durable LVAD therapy are often evaluated using INTERMACS Profiles, which help specialists estimate the urgency of mechanical circulatory support based on the severity of advanced heart failure. Selection for durable mechanical circulatory support requires a comprehensive multidisciplinary evaluation. The Heart Team evaluates not just heart function, but also kidney/liver health, infection risk, nutritional status, family support, and the patient’s ability to manage complex equipment safely at home.
Types of Mechanical Circulatory Support Devices
There are several classes of MCS devices, ranging from balloon pumps that indirectly assist blood flow to total artificial hearts that completely replace the native ventricles.
Key Takeaway: No single device fixes every problem; your cardiologist selects the specific technology that matches which side of your heart is failing and how urgently support is needed.
Detailed Explanation
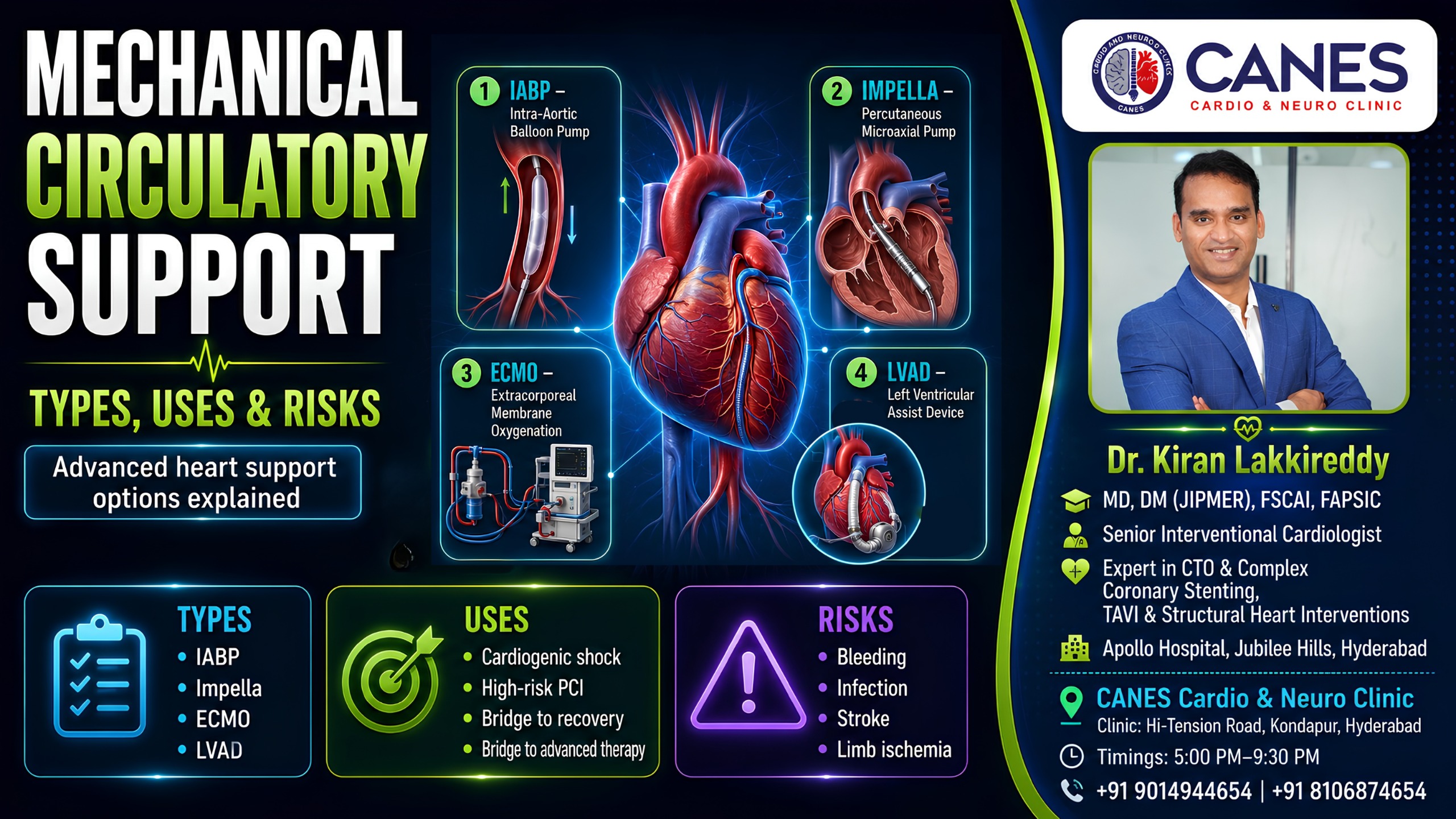
Intra-Aortic Balloon Pump (IABP): A temporary device containing a balloon positioned in the aorta. It inflates when the heart relaxes and deflates when it contracts, improving blood flow to the coronary arteries while reducing the heart’s workload.
Percutaneous Ventricular Assist Devices: Inserted through a blood vessel, these actively pump blood from a heart chamber into a major artery. They provide more circulatory assistance than an IABP but carry risks like vascular injury.
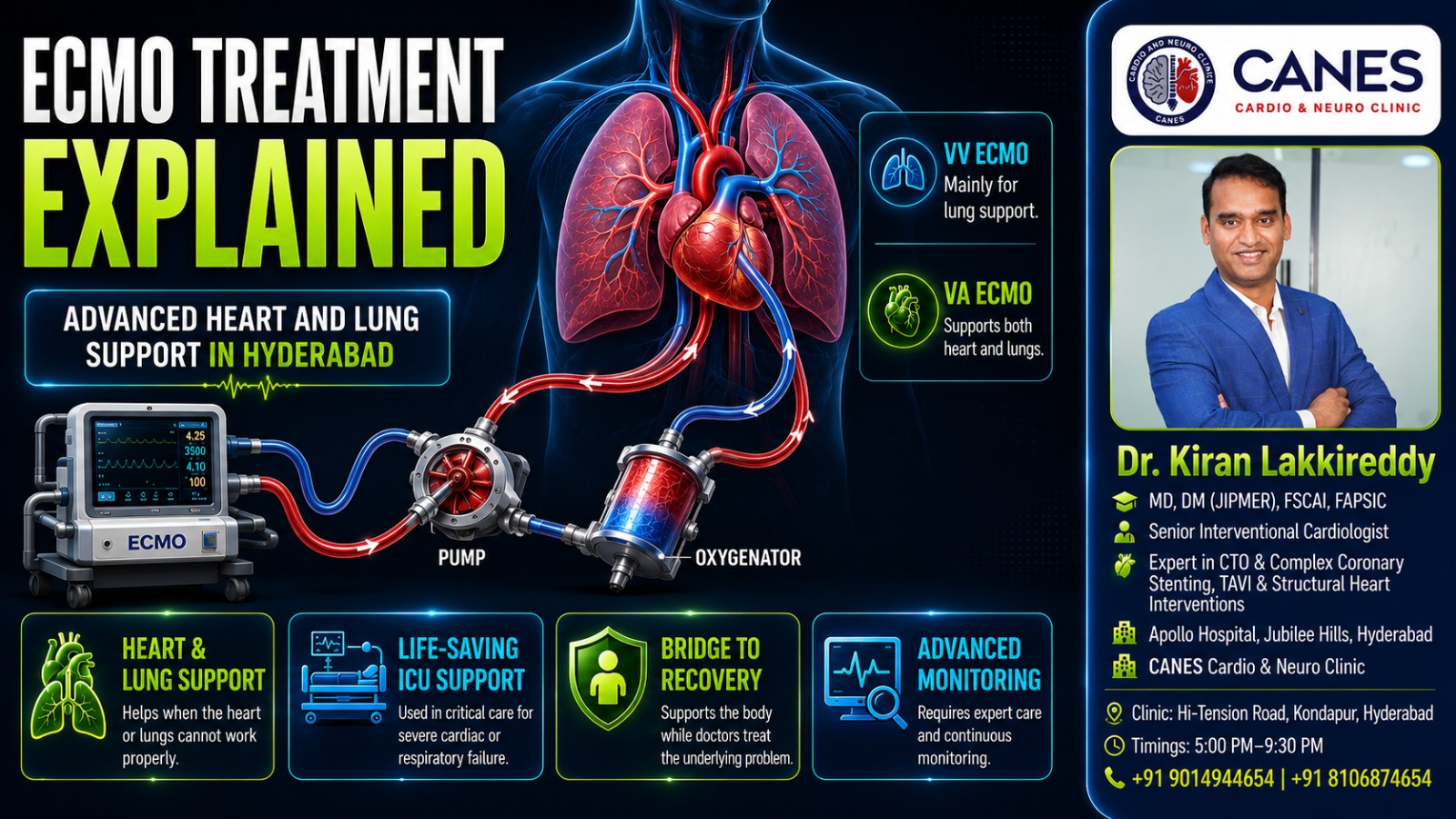
Extracorporeal Membrane Oxygenation (ECMO): Circulates blood through an external oxygenator. VA-ECMO supports both circulation and the lungs for profound shock. VV-ECMO supports only the lungs. ECMO creates vital time for recovery but requires continuous intensive care monitoring.
Left Ventricular Assist Device (LVAD): A durable mechanical pump implanted near the heart that takes over the workload of the weakened left ventricle. It includes a driveline passing through the skin to an external power source.
Right Ventricular Assist Device (RVAD): Supports the right ventricle in moving blood toward the lungs, often used after a severe right-sided heart attack or when the right heart fails after LVAD implantation.
Biventricular Assist Devices (BIVAD): Required when neither side of the heart can maintain circulation. This is highly complex and requires careful balancing of blood flow.
Total Artificial Heart (TAH): Replaces both native ventricles and their valves entirely. It is primarily used as a temporary bridge to transplantation in patients facing imminent risk from irreversible biventricular failure.
Decision Support: "Bridge" and "Destination Therapy"
Mechanical circulatory support is classified by its ultimate clinical goal, whether that is bridging a patient to natural recovery, keeping them alive until a transplant, or serving as a permanent destination therapy.
Treatment Strategies
Strategy | What It Means for the Patient |
|---|---|
Bridge to Recovery | Temporary support is provided while doctors treat a potentially reversible condition. |
Bridge to Decision | Creates time to evaluate organ function, brain status, and future treatment options. |
Bridge to Transplantation | The device maintains circulation while an eligible patient waits for a donor heart. |
Bridge to Candidacy | Support allows general health to improve enough for the patient to become eligible for a transplant. |
Destination Therapy | A durable device (like an LVAD) is used as long-term treatment when transplantation is not an option. |
(Note: The intended strategy may change. A patient initially deemed too unwell for a transplant may improve on LVAD support and later become eligible.)
What Are the Risks of Mechanical Circulatory Support?
Mechanical circulatory support can be lifesaving, but it carries severe risks including major bleeding, blood clots, life-threatening infections, vascular complications, and device malfunction.
Key Takeaway: Because these devices interact directly with your bloodstream and rely on external power, they require continuous, lifelong monitoring to prevent catastrophic complications.
Detailed Explanation
While the benefits often outweigh the risks in life-or-death scenarios, complications must be closely managed:
Bleeding: Large catheters, surgery, and required anticoagulant medicines (blood thinners) heavily increase the risk of bleeding in the chest, digestive tract, or brain.
Blood Clots and Stroke: Blood contacting artificial surfaces can easily form clots. If a clot travels to the brain, it can cause a devastating stroke.
Infection: Temporary cannulas and durable LVAD drivelines passing through the skin create entry points for bacteria. Infection prevention is a daily necessity.
Device Malfunction: Pumps, controllers, or batteries can fail. Patients with durable devices must carry backup equipment and be rigorously trained in emergency alarm management.
Right-Heart Failure: After an LVAD unloads the left ventricle, the right ventricle must work harder to push blood through the lungs. A weak right ventricle may fail under this new pressure.
Who May Not Be Suitable for Mechanical Support?
MCS is not suitable for patients with irreversible severe brain injury, advanced multi-organ failure, uncontrolled bleeding, or those lacking the necessary caregiver support to safely manage complex equipment at home.
Key Takeaway: The presence of severe heart failure does not automatically mean a device will help; the team must ensure there is a realistic pathway to a meaningful quality of life.
Detailed Explanation
Certain factors make mechanical circulatory support unsafe or unlikely to succeed. These include systemic infections that cannot be controlled, vascular anatomy that prevents safe device insertion, or a terminal condition that cannot be bridged to a meaningful treatment goal. Furthermore, because a durable LVAD requires meticulous daily maintenance, an inability to manage the device safely without adequate family or caregiver support is a major contraindication.
Myth vs. Fact: Mechanical Circulatory Support
Understanding the realities of advanced heart devices helps patients and families make informed, rational decisions during a crisis.
Common Myth | Medical Fact |
|---|---|
MCS is exactly the same thing as a pacemaker. | A pacemaker only controls heart rhythm. MCS devices actively assist or completely replace the heart’s physical pumping function. |
Every patient with severe heart failure gets an LVAD. | Implantation is only considered after an extensive assessment of surgical risk, right-heart function, and long-term viability. |
ECMO cures heart failure permanently. | ECMO temporarily supports circulation to provide time for recovery; it does not cure the underlying disease. |
If I get an LVAD, I don’t need heart medications anymore. | Blood thinners (anticoagulants) and other cardiac medicines remain absolutely essential and must be taken exactly as prescribed. |
Actionable Checklist: What to Ask the Heart Team
Before proceeding with mechanical circulatory support, patients or their relatives must gather clear information. Use this checklist when speaking with your doctors:
[ ] Identify the Failure: Ask, “Which specific part of the heart is failing, and why is this specific device being recommended?”
[ ] Clarify the Goal: Ask, “Is our current goal recovery, a bridge to a transplant, or long-term destination therapy?”
[ ] Understand the Risks: Ask, “What are the most important, immediate risks for this individual patient?”
[ ] Plan for the Future: Ask, “What happens if the native heart does not recover as expected?”
[ ] Prepare for Home Care: Ask, “What specific training and daily caregiver support will our family need to provide if the patient comes home?”
Advanced Cardiac Evaluation at CANES Clinic
A discussion about mechanical circulatory support often begins after a patient has experienced repeated heart-failure admissions or a serious episode of cardiac instability.
At CANES Cardio & Neuro Clinic, the focus is on clear patient education, detailed cardiovascular assessment, and shared decision-making. The clinic is guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist specializing in complex cardiology.
Mechanical circulatory support particularly ECMO, durable LVAD implantation, BIVAD support, and total artificial heart surgery requires hospital-based multidisciplinary care. A cardiovascular consultation can help patients understand their condition, review available reports, and determine whether advanced heart-failure or surgical evaluation is needed.
Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Road, Kondapur, Hyderabad
Contact: +91 9014944654
Appointment Booking: Visit CANES Clinic Official Portal
Specialist Profile: Dr. Kiran Lakkireddy Official Website
(Note: Patients experiencing symptoms of cardiogenic shock—severe breathlessness, fainting, cold/clammy hands—should go directly to an emergency department rather than waiting for a scheduled clinic consultation.)
Key Points to Remember
MCS Supports Circulation: It helps the heart deliver blood when pumping function is critically reduced.
Devices Are Not Interchangeable: IABP, percutaneous VADs, VA-ECMO, LVAD, and total artificial hearts provide vastly different levels and types of support.
Temporary vs. Durable: Temporary devices support recovery or decision-making; durable LVADs may remain in place for years.
Patient Selection Is Critical: Organ function, recovery potential, bleeding risk, and long-term goals strongly dictate the decision.
MCS Carries Serious Risks: Bleeding, infection, clots, stroke, and device malfunction require lifelong, close monitoring.
Multidisciplinary Care Is Essential: Device placement and management require a highly experienced Heart Team.
Frequently Asked Questions (FAQs)
Mechanical circulatory support is one specific form of life-sustaining treatment designed to assist blood circulation. Some advanced systems, like VA-ECMO, also support oxygenation and act as full cardiopulmonary life support.
Recovery is possible when the underlying condition is reversible, such as in selected cases of myocarditis or acute cardiomyopathy. Recovery is highly unlikely in irreversible end-stage heart failure.
VA-ECMO supports both circulation and the lungs, actively assisting the heart. VV-ECMO supports only gas exchange for the lungs and does not provide direct heart pumping support.
Yes. Selected patients with a durable LVAD can return home after recovering from surgery and completing rigorous device-management and safety training.
An LVAD simply assists the weakened left ventricle while your native heart remains inside your chest. A total artificial heart requires surgically removing both native ventricles and their valves to completely replace them.
No. Suitability depends entirely on the cause of heart failure, liver and kidney function, surgical risk, expected recovery, transplant eligibility, and the patient’s personal treatment goals.
No. Some devices, such as durable LVADs, may provide long-term support, but they do not replace a heart transplant in every patient. For eligible individuals with irreversible end-stage heart failure, transplantation remains the preferred definitive treatment.

Expert Care
Hyderabad's leading Cardio & Neuro specialists.
