Why Chronic Total Occlusions (CTOs) Need to Be Opened: An Evidence-Based Perspective
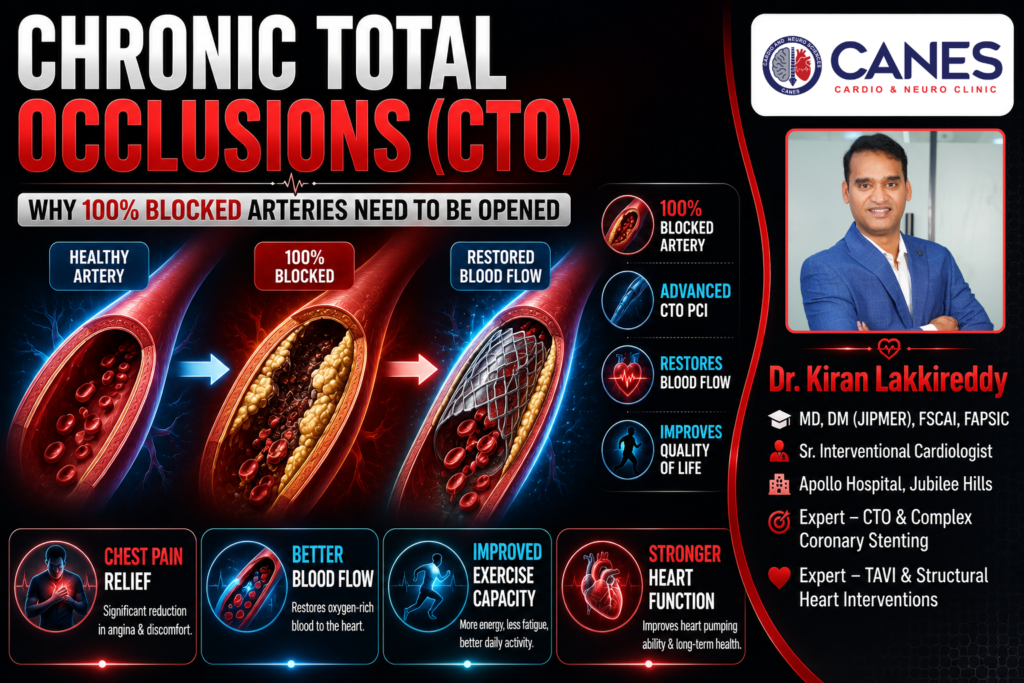
● Lifestyle & Prevention Why Chronic Total Occlusions (CTOs) Need to Be Opened: An Evidence-Based Perspective Table of Contents Introduction What Exactly Are Chronic Total Occlusions? Why Should Chronic Total Occlusions Be Opened? What Happens If Chronic Total Occlusions Are Not Opened? Which CTOs Should Be Opened? Who May Not Benefit From CTO PCI? What Investigations Are Required Before Opening a CTO? Actionable Checklist: What Should You Do Next? Expert CTO Interventions at CANES Clinic FAQs Book a Consultation Prevention is better than cure. Talk to our specialists today. Book Now Receiving a diagnosis of a completely blocked heart artery can sound terrifying, but modern cardiology has evolved significantly to treat complex conditions. A Chronic Total Occlusion (CTO) is a complete blockage of a coronary artery that has been present for at least three months. Unlike sudden blockages that cause acute heart attacks, Chronic Total Occlusions develop gradually. Because they grow slowly, your body attempts to adapt by forming tiny, fragile detour blood vessels called collaterals to bypass the blockage. However, these collateral vessels are rarely enough. When you walk, exercise, or experience stress, these small detour pathways cannot deliver enough oxygen-rich blood to your heart muscle. As a result, patients frequently experience severe chest pain, extreme fatigue, and a progressive deterioration of their overall heart function. At CANES Cardio & Neuro Clinic in Hyderabad, guided by Dr. Kiran Lakkireddy, we specialize in advanced interventional cardiology. Today, a highly specialized procedure known as CTO Percutaneous Coronary Intervention (CTO PCI) can safely and successfully open these chronic blockages. In this comprehensive, evidence-based guide, we will explore exactly why opening Chronic Total Occlusions is necessary, who benefits the most, and who might safely avoid the procedure. Quick Answer Chronic Total Occlusions are 100% blocked arteries that have been closed for months or years, causing the heart to starve for oxygen. Opening a CTO using a specialized stenting procedure (CTO PCI) restores essential blood flow to the heart muscle. This minimally invasive procedure significantly relieves chest pain, improves your ability to exercise, protects your long-term heart function from deteriorating, and dramatically improves your overall quality of life. What Exactly Are Chronic Total Occlusions? Chronic Total Occlusions are 100% complete blockages in a main coronary artery that have existed for more than 90 days, typically composed of heavily calcified, hardened cholesterol plaque. Key Takeaway: A CTO is a long-standing, hardened roadblock in your artery that forces your heart to rely on inefficient, temporary detour vessels for blood supply. Quick Answer To understand Chronic Total Occlusions, imagine a major highway that has been completely blocked by a landslide for months. Over time, drivers start using small, unpaved backroads to get around the blockage. In your heart, these backroads are called “collateral vessels.” While these collaterals are an amazing natural defense mechanism that keeps the heart muscle alive, they are fundamentally inadequate. They are too small to carry the high volume of blood your heart needs when it works hard. As a result, the heart muscle supplied by the blocked artery remains alive but “hibernating” it is constantly starving for oxygen, which causes symptoms like severe breathlessness and chest pain (angina) during physical exertion. Why Should Chronic Total Occlusions Be Opened? The primary goal of a CTO PCI procedure is to eliminate the roadblock and restore normal, high-volume blood flow to the deprived heart muscle, which immediately improves symptoms and long-term cardiac function. Key Takeaway: Opening a CTO wakes up hibernating heart muscle, drastically improving your daily energy levels and reducing your dependence on temporary collateral vessels. Quick Answer Advances in interventional cardiology mean that experienced centers now achieve success rates exceeding 85–95% for CTO PCI. Revascularization (opening the artery) provides several evidence-based clinical benefits: Relief of Angina and Symptoms: Patients with a CTO frequently experience severe chest pain, reduced exercise capacity, and profound fatigue. Multiple randomized clinical trials have proven that successful CTO revascularization significantly reduces angina frequency and improves daily physical functioning. Improvement in Left Ventricular Function: The heart muscle below the blockage is often viable but functionally paralyzed (hibernating myocardium). Restoring normal blood flow wakes this tissue up, improving the heart’s overall pumping strength (Left Ventricular Ejection Fraction) and stopping the heart from dangerously enlarging. Reduction in Ischemic Burden: Opening the main artery physically reduces the total area of the heart that is starving for oxygen (ischemia). Patients with a large ischemic burden derive the absolute greatest survival benefit from this procedure. Improved Quality of Life: The most immediate and profound benefit reported by patients is a massive upgrade in their quality of life. Patients can return to physical activity, experience less breathlessness, and significantly reduce their daily anti-anginal medications. What Happens If Chronic Total Occlusions Are Not Opened? Leaving significant Chronic Total Occlusions untreated often leads to a progressive worsening of daily chest pain, dangerous weakening of the heart muscle, and a significantly higher risk of developing congestive heart failure. Key Takeaway: While collaterals keep the muscle alive temporarily, relying on them long-term causes the heart muscle to scar, weaken, and eventually fail. Quick Answer Ignoring a significant blockage that is actively starving a large portion of the heart carries severe long-term consequences: Progressive Heart Failure: Long-standing oxygen deprivation causes the heart muscle to develop irreversible scar tissue (fibrosis). The heart compensates by remodeling and stretching out, which eventually leads to congestive heart failure. Ventricular Arrhythmias: Scarred, ischemic heart tissue becomes highly unstable. This acts as an arrhythmogenic substrate, meaning it can trigger dangerous, chaotic heart rhythms (like ventricular tachycardia) that can lead to sudden cardiac death. Greater Dependence on Collaterals: Collateral circulation often looks impressive on an angiogram but rarely provides normal perfusion. Over time, if these tiny collateral vessels fail or become diseased themselves, the dependent heart muscle will inevitably die. Which CTOs Should Be Opened? International cardiology guidelines recommend CTO PCI in carefully selected patients, particularly those with persistent symptoms, demonstrable ischemia, and viable myocardium. Key Takeaway: Careful patient selection is the most critical step; the procedure is
