ECMO: Understanding Advanced Heart and Lung Life Support
Table of Contents
- Introduction
- What Is ECMO?
- How Does an ECMO Machine Work?
- What Is the Difference Between VA-ECMO and VV-ECMO?
- Who May Not Benefit From ECMO?
- Decision Support: Is ECMO a Last-Resort Treatment?
- How Long Can a Patient Remain on ECMO?
- What Are the Possible Risks of ECMO?
- Myth vs. Fact: Understanding ECMO
- What Should You Do Next? (A Checklist for Families)
- Advanced Cardiovascular Evaluation at CANES Clinic
- FAQs
Book a Consultation
Prevention is better than cure. Talk to our specialists today.
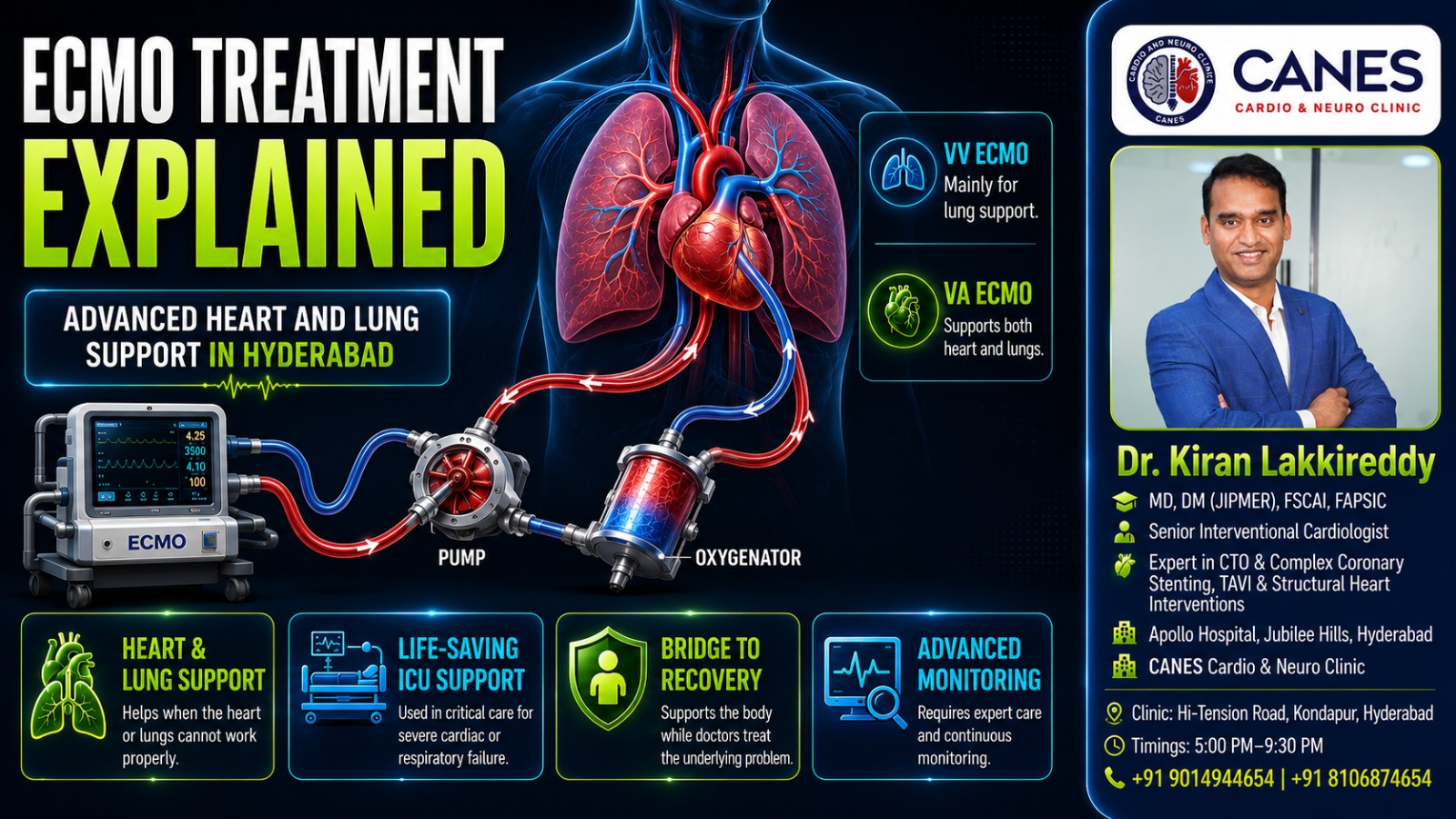
Severe heart or lung failure can prevent the body from receiving enough oxygen, even when doctors use maximum medical therapy, mechanical ventilation, and other intensive care treatments. In carefully selected, critically ill patients, ECMO life support may temporarily perform part of the work of the heart, lungs, or both organs.
ECMO stands for Extracorporeal Membrane Oxygenation. “Extracorporeal” means outside the body. During treatment, blood is removed through large tubes called cannulas, circulated through an external machine, supplied with oxygen, cleared of carbon dioxide, and safely returned to the patient. It is crucial to understand that ECMO does not cure heart or lung disease. Its exact purpose is to maintain circulation and oxygen delivery while the medical team treats the underlying condition, evaluates recovery, or prepares the patient for another life-saving intervention.
At CANES Cardio & Neuro Clinic, a specialized cardiovascular care center in Hyderabad, our approach emphasizes clear patient education, careful cardiovascular assessment, and shared decision-making. Guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist specializing in complex cardiology, we help patients and families navigate serious cardiac conditions and determine when advanced hospital-based care is required.
Quick Answer
ECMO life support is a temporary, highly advanced system that circulates blood outside the body, adds oxygen, removes carbon dioxide, and returns the blood to the patient. There are two principal forms: VA-ECMO (which supports both the heart and lungs) and VV-ECMO (which supports the lungs but does not directly pump for the heart). ECMO is utilized when potentially reversible heart or lung failure remains life-threatening despite maximum conventional treatments.
ECMO Life Support at a Glance
Feature | What It Means | Why It Matters |
|---|---|---|
Extracorporeal Circulation | Blood travels temporarily outside the body through an external circuit. | The machine can oxygenate the blood and, in VA-ECMO, heavily support circulation. |
Membrane Oxygenator | A component that adds oxygen and removes carbon dioxide. | It performs part of the gas-exchange work normally carried out by the natural lungs. |
VA-ECMO / VV-ECMO | Artery/Vein configurations for returning blood to the body. | VA supports both the heart and lungs; VV supports severe lung failure only. |
Temporary Support | ECMO is usually continued for days or weeks rather than permanently. | It provides essential time for recovery, transplantation assessment, or definitive surgery. |
What Is ECMO?
Extracorporeal membrane oxygenation (ECMO) is an advanced form of temporary cardiopulmonary life support used when the heart, lungs, or both organs completely fail to meet the body’s metabolic needs.
Key Takeaway: ECMO supports the patient while another treatment or the body’s natural healing process addresses the underlying disease; it is a bridge to recovery, not a cure in itself.
Detailed Explanation
The ECMO circuit acts in some ways like a modified heart-lung bypass system. However, unlike the bypass machine used for a limited period during open-heart surgery, ECMO may remain in continuous use for days or weeks under strict intensive-care monitoring.
Depending on the specific configuration, ECMO life support can add oxygen to the blood, remove carbon dioxide, maintain blood flow to vital organs, and vastly reduce the workload placed on injured lungs. When the heart is severely weakened, it can support circulation to keep the patient alive, acting as a crucial bridge to a ventricular assist device (VAD), transplantation, or natural recovery.
How Does an ECMO Machine Work?
An ECMO machine creates a controlled external circuit where oxygen-depleted blood is continuously drained through large cannulas, pumped through a membrane oxygenator for gas exchange, warmed, and safely returned to the patient.
Key Takeaway: The machine artificially replicates the most vital functions of your heart and lungs, requiring continuous, meticulous calibration by a specialized intensive care team.
Detailed Explanation
The process relies on a highly sophisticated, continuous loop. First, one or more large tubes called cannulas are placed in major blood vessels in the groin or neck (Cannulation). Low-oxygen blood is drawn from the venous circulation into the ECMO circuit.
A mechanical centrifugal pump then moves this blood through a membrane oxygenator, often described as an artificial lung. Here, oxygen enters the blood across a membrane while carbon dioxide is extracted. A heat exchanger warms the blood back to an appropriate body temperature before it is forcefully returned to the patient’s body either into a vein (VV-ECMO) or an artery (VA-ECMO). The circuit is monitored continuously because any changes in pressure, flow, oxygenation, or the appearance of clots require an immediate, expert response.
What Is the Difference Between VA-ECMO and VV-ECMO?
Venoarterial (VA) ECMO removes blood from a vein and returns it to an artery to support both the heart and lungs, whereas Venovenous (VV) ECMO removes and returns blood solely to the venous system to support only the lungs.
Key Takeaway: If a patient’s heart is failing, they require VA-ECMO. If their heart pumps fine but their lungs are failing, they require VV-ECMO.
Detailed Explanation
In VA-ECMO, because the oxygenated blood is returned to the arterial circulation under mechanical flow, the machine takes over the pumping action of the heart. It is considered for severe cardiac failure (like cardiogenic shock), particularly when circulation remains inadequate despite strong medicines and IV fluids.
In VV-ECMO, the patient’s own heart must still pump the freshly oxygenated blood throughout the body. Therefore, VV-ECMO supports severe, acute respiratory failure (such as severe pneumonia or ARDS) but does not directly provide the same circulatory assistance or blood pressure support as VA-ECMO.
Comparing ECMO Configurations
Consideration | VA-ECMO | VV-ECMO |
|---|---|---|
Primary Purpose | Heart and lung support | Lung support only |
Blood Returned To | An artery | A vein |
Supports Blood Pressure? | Yes | No |
Heart Function Required | May be profoundly impaired | Must be adequate to circulate blood |
Common Clinical Setting | Cardiogenic shock or cardiac arrest | Severe reversible respiratory failure |
Who May Not Benefit From ECMO?
ECMO may not provide meaningful benefit for patients with irreversible severe brain injury, advanced multiorgan failure, uncontrolled bleeding, or terminal illnesses where there is no realistic pathway to recovery or transplantation.
Key Takeaway: ECMO is an incredibly invasive therapy; if a patient has no viable pathway off the machine, placing them on life support only prolongs suffering without offering a cure.
Detailed Explanation
Patient selection is critical. ECMO is only considered when the expected benefit of temporary support heavily outweighs its substantial risks. Many ECMO programs follow guidance developed by the Extracorporeal Life Support Organization (ELSO) to support patient selection, monitoring, and quality improvement. It requires a realistic “exit strategy.”
Factors that make ECMO unsuitable or extremely high risk include severe vascular disease that prevents safe cannula insertion, major contraindications to blood thinners (anticoagulation), or irreversible heart/lung failure in a patient who is not a candidate for an organ transplant. The medical team makes these difficult decisions based on the patient’s complete condition and the ultimate intended goal of the support.
Decision Support: Is ECMO a Last-Resort Treatment?
While ECMO life support is an advanced rescue therapy, waiting to use it as an absolute “last resort” after severe, irreversible organ damage has already occurred significantly reduces the patient’s chances of survival.
The appropriate timing requires a delicate clinical balance. Starting it too early exposes a patient to major bleeding and stroke risks without sufficient benefit. However, starting it too late prevents recovery. It is frequently described by the goal it is intended to achieve, known as a “bridge.”
The "Bridge" Strategy in ECMO
ECMO Strategy | What It Means for the Patient |
|---|---|
Bridge to Recovery | Support continues while a reversible heart or lung condition heals. |
Bridge to Decision | Creates time to evaluate recovery potential, brain status, and future options. |
Bridge to Transplant | Maintains the patient while they await a donor heart or lungs. |
Bridge to Durable Support | Stabilizes circulation before transitioning to an implantable heart pump (LVAD). |
How Long Can a Patient Remain on ECMO?
ECMO is intended as temporary support. Some patients require only a few days, while others may remain on ECMO life support for several weeks. The duration depends on the underlying illness, recovery progress, and whether ECMO is serving as a bridge to recovery, transplantation, or another advanced therapy.
Key Takeaway: There is no strict time limit, but ECMO is not permanent. It must continually serve a realistic, achievable medical goal.
Detailed Explanation
The exact number of days a patient remains on the machine varies drastically. If the heart or lungs show clear signs of healing, the intensive care team will begin “weaning” trials temporarily turning down the ECMO support to test if the patient’s own organs can handle the workload. If the patient is waiting for a lung or heart transplant, they may remain on support until donor organs become available. Throughout this time, the medical team continuously assesses whether the treatment is still providing a meaningful clinical benefit.
What Are the Possible Risks of ECMO?
Because it is one of the most complex treatments used in critical care, ECMO life support carries significant risks, including severe bleeding, blood clots, life-threatening infections, limb ischemia, and devastating neurological injury like a stroke.
Key Takeaway: A patient’s risk depends on how sick they were before ECMO started and how long they must remain on the machine. Continuous intensive care monitoring is mandatory.
Detailed Explanation
Bleeding is among the most frequent complications because patients require constant anticoagulation (blood thinners) while having large plastic cannulas sitting in their major blood vessels. Bleeding inside or around the brain is particularly serious.
Conversely, clots can form in the artificial oxygenator or pump. Patients are continuously monitored using blood tests to balance the competing risks of bleeding and clotting. If an air bubble or clot enters the patient’s circulation, it can cause a massive stroke. Additionally, inserting large tubes into the femoral (leg) artery during VA-ECMO can severely reduce blood flow down the leg, leading to limb ischemia, which threatens the muscles and nerves. The ECMO circuit itself can also damage red blood cells (haemolysis) or suffer mechanical failure, requiring immediate expert replacement.
Myth vs. Fact: Understanding ECMO
Understanding the realities of ECMO life support helps families make informed, rational decisions during a crisis.
Common Myth | Medical Fact |
|---|---|
ECMO cures heart or lung failure. | ECMO only provides temporary support while the underlying illness is treated or natural recovery occurs. |
A patient on ECMO no longer needs a ventilator. | Many patients continue to receive mechanical ventilation, often with gentler settings to let the lungs rest. |
Starting ECMO guarantees survival. | ECMO creates an opportunity for recovery but cannot reverse every illness or prevent every complication. |
ECMO can continue indefinitely. | It is strictly temporary support and should continue only while it serves a realistic, achievable treatment goal. |
What Should You Do Next? (A Checklist for Families)
Having a loved one placed on ECMO life support is an incredibly stressful experience. Families should request regular, understandable updates. Use this checklist of questions to ask the ECMO Intensive Care team:
Clarify the Type: Ask, “Is the patient receiving VA-ECMO (Heart & Lungs) or VV-ECMO (Lungs only)?”
Determine the Goal: Ask, “Is our current goal a bridge to recovery, a bridge to a transplant, or a bridge to a decision?”
Monitor Progress: Ask, “What specific daily signs or lab results will show us that the patient is actually improving?”
Understand the Exit Strategy: Ask, “How will the medical team test whether the ECMO support can be safely reduced or removed?”
Advanced Cardiovascular Evaluation at CANES Clinic
ECMO life support is an emergency, hospital-based treatment requiring an appropriately equipped intensive-care unit, trained ECMO personnel, and immediate access to cardiothoracic surgeons. It is not an outpatient procedure.
At CANES Cardio & Neuro Clinic, patients and families can receive structured cardiovascular evaluation and guidance regarding serious heart conditions, including advanced heart failure, cardiogenic shock risk, and the need for referral to higher-level hospital care.
Guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist specializing in complex cardiology, our focus is on detailed assessment, understandable communication, and appropriate coordination with advanced cardiac or surgical teams when necessary.
Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Road, Kondapur, Hyderabad
Contact: +91 9014944654
Appointment Booking: Visit CANES Clinic Official Portal
Specialist Profile: Dr. Kiran Lakkireddy Official Website
(Note: A person with severe breathlessness, chest pain, confusion, fainting, blue lips, or loss of consciousness requires immediate emergency hospital care rather than a routine clinic appointment.)
Key Points to Remember
ECMO Temporarily Supports Vital Functions: It can support just the lungs (VV-ECMO) or both the heart and lungs (VA-ECMO).
ECMO Is Not a Cure: It creates vital time for medical treatment, natural recovery, or transition to another intervention like a transplant.
Patient Selection Is Critical: The underlying condition must have a realistic recovery or treatment pathway for ECMO to be ethically and medically appropriate.
Complications Can Be Severe: Bleeding, clotting, infection, stroke, vascular injury, and mechanical circuit problems require continuous, 24/7 monitoring.
Daily Reassessment Is Essential: Doctors repeatedly evaluate whether support can be safely reduced, continued, or transitioned to a new strategy.
Frequently Asked Questions (FAQs)
ECMO stands for Extracorporeal Membrane Oxygenation. It describes a medical system that moves blood outside the body through an artificial oxygenator before returning it to the circulation.
ECMO is one of the most advanced forms of temporary cardiopulmonary life support available in modern intensive care. It assists gas exchange and circulation, but patients typically also require a mechanical ventilator, dialysis, continuous IV medicines, and nutritional support.
Not usually. The native heart commonly continues beating. VA-ECMO reduces the amount of circulation the heart must forcefully provide, allowing the stressed muscle to rest, but the degree of native cardiac activity varies.
ECMO can perform a substantial amount of oxygenation and carbon dioxide removal, but the natural lungs remain in the body and continue receiving treatment. The goal is to drastically reduce their workload so they can heal.
Cannulation (inserting the tubes) is performed under anesthesia or heavy sedation. Patients usually receive continuous pain control and sedation, although these medicines may be lightened when the patient’s vital signs stabilize.
Some highly stable patients can be awake, communicate, and occasionally even participate in active physical rehabilitation (like walking) while on ECMO. However, this is only attempted with strict, specialized supervision.
There is no single survival rate. The outcome depends entirely on the patient’s age, diagnosis, ECMO type, duration of illness before ECMO started, and any complications. Population statistics cannot reliably predict an individual’s outcome.
Yes. Selected, eligible patients may receive ECMO life support while being evaluated for or actively awaiting a donor heart or lung transplantation.

Expert Care
Hyderabad's leading Cardio & Neuro specialists.
