What Is Motor Neurone Disease? Understanding the Causes, Symptoms, Diagnosis, and Treatment
Table of Contents
- Introduction
- 1. What Is Motor Neurone Disease?
- 2. Is MND the Same as ALS?
- 3. What Are the First Signs of MND?
- 4. When Should You Seek Medical Attention for Possible MND?
- 5. Why Does MND Cause Muscle Weakness?
- 6. What Causes MND?
- 7. Is MND Hereditary?
- 8. How Is MND Diagnosed?
- 9. Can MND Be Prevented or Cured?
- 10. How Long Can Someone Live With MND?
- FAQs
Book a Consultation
Prevention is better than cure. Talk to our specialists today.
Experiencing unexplained muscle weakness, muscle twitching, or subtle changes in speech can be deeply concerning. The human nervous system relies on a continuous, uninterrupted exchange of electrical signals to coordinate everyday actions. When these communication pathways begin to degrade, simple tasks like gripping an object or walking on a flat surface can become increasingly difficult. Securing a comprehensive evaluation from a medical professional is the most critical step in identifying the root cause of these neurological changes and establishing an evidence-based management plan.
Quick Answer :
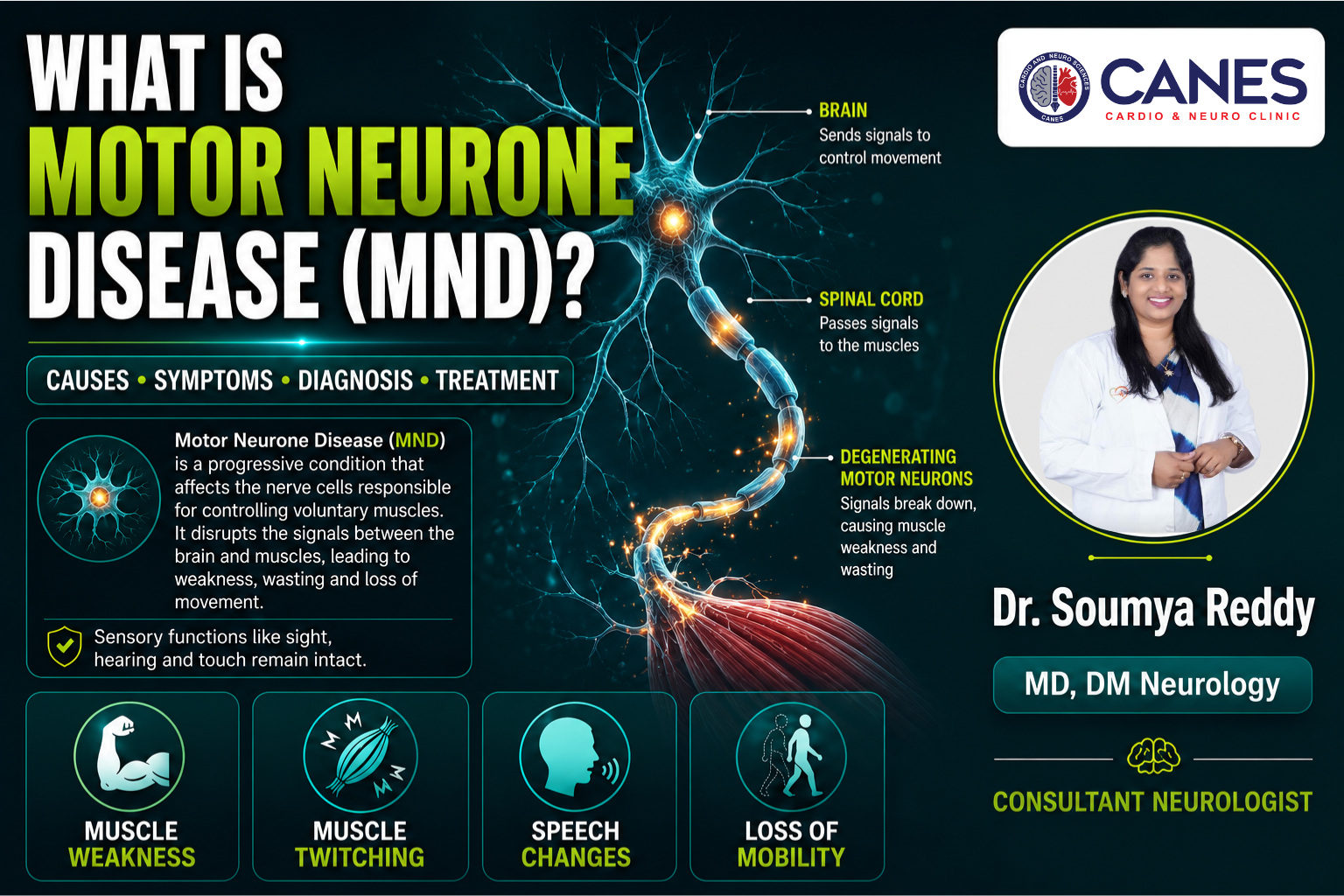
Motor Neurone Disease (MND) is a progressive neurodegenerative disorder that systematically destroys the nerve cells responsible for voluntary muscle movement. The condition interrupts the electrical signals between the brain and muscles, leading to muscle wasting, weakness, loss of mobility, and eventual respiratory challenges. While there is currently no cure, advanced diagnostics and multidisciplinary care significantly improve symptom management and quality of life.
1. What Is Motor Neurone Disease?
Motor Neurone Disease (MND) is a group of progressive neurological disorders that selectively destroy motor neurons, the specialized nerve cells controlling voluntary muscle movements. As these neurons degenerate, the brain loses its ability to communicate with muscles, resulting in muscle weakness, wasting (atrophy), and difficulties with speaking, swallowing, and breathing.
Key Takeaway: Motor Neurone Disease targets the nerve cells that control voluntary movement, cutting off communication between the brain and the muscular system, while leaving sensory functions like sight and touch intact.
1. Detailed Explanation
To understand this neurodegenerative disorder, it helps to examine the anatomy of the nervous system. Voluntary movements such as walking, lifting objects, and talking require a two-part nerve pathway:
Upper Motor Neurons: These cells are located in the brain and send electrical instructions down through the spinal cord.
Lower Motor Neurons: These cells accept the signals in the spinal cord and extend outward to directly stimulate muscle tissue.
In an individual with Motor Neurone Disease, both upper and lower motor neurons gradually break down and die. When these cells degenerate, the vital electrical messages can no longer span the anatomical gap. Starved of stimulation, the muscles begin to weaken and naturally shrink over time. Crucially, because MND specifically attacks motor pathways, the sensory nervous system remains fully functional; a patient’s ability to see, hear, smell, taste, and feel physical touch on the skin is entirely preserved.
2. Is MND the Same as ALS?
Amyotrophic Lateral Sclerosis (ALS) is the most common and widespread form of Motor Neurone Disease, but it is not the only type. While the terms are often used interchangeably in casual conversation or general media, MND is the broader umbrella medical classification that includes several other distinct neurological variants.
Key Takeaway: ALS is a specific type of Motor Neurone Disease that damages both upper and lower motor neurons, representing the vast majority of all global MND diagnoses.
1. Detailed Explanation
In medical terms, Motor Neurone Disease acts as a category heading. Amyotrophic Lateral Sclerosis accounts for approximately 85% to 90% of all cases within this category. In ALS, the degeneration occurs simultaneously in both the upper motor neurons of the brain and the lower motor neurons of the spinal cord, leading to widespread physical weakness that affects the limbs, speech, and respiratory system.
However, other variants exist depending on which specific parts of the motor pathway are affected. To understand the different types of conditions that fall under the MND umbrella, review the clinical comparison table below:
MND Classifications: ALS vs. PLS vs. PMA vs. PBP
| Feature | Amyotrophic Lateral Sclerosis (ALS) | Primary Lateral Sclerosis (PLS) | Progressive Muscular Atrophy (PMA) | Progressive Bulbar Palsy (PBP) |
| Neurons Affected | Both Upper and Lower | Upper Motor Neurons only | Lower Motor Neurons only | Brainstem Bulbar Neurons |
| Primary Symptoms | Muscle weakness, wasting, and stiffness | Extreme muscle stiffness, slow movement, spasticity | Muscle wasting, weakness, and deep twitching | Difficulty speaking, slurred speech, choking |
| Onset Location | Usually limbs (arms or legs) | Usually begins in both legs | Usually begins in hands or feet | Muscles of the throat and tongue |
| Progression Rate | Rapid to moderate | Slow, non-fatal variant | Slower progression than ALS | Rapid, affects breathing early |
3. What Are the First Signs of MND?
The first signs of Motor Neurone Disease typically manifest as mild, painless, and asymmetrical muscle weakness, such as an unstable hand grip, frequent tripping, or slurred speech. Because these initial physical changes develop gradually, they are frequently mistaken for minor nerve compressions, fatigue, or normal signs of aging.
Key Takeaway: Early signs of MND are usually subtle and localized, often presenting as a weak grip in one hand, foot drop in one leg, or minor changes in vocal clarity.
1. Detailed Explanation
Because the early signs of motor neurone disease are painless and isolated, many individuals do not immediately recognize the need for a neurological assessment. Clinical observation shows that symptoms usually begin in one of three distinct anatomical regions:
The Arms (Limb Onset): Patients may notice an unexpected weakness in their dominant hand. Everyday fine motor tasks, such as fastening buttons, turning keys, opening jars, or writing legibly, become increasingly challenging.
The Legs (Limb Onset): Weakness often presents as “foot drop,” where the muscles responsible for lifting the front of the foot weaken. This causes the toes to drag on the ground, leading to unexplainable stumbling or tripping over completely flat surfaces.
The Throat and Mouth (Bulbar Onset): The muscles controlling speech and swallowing are affected first. A patient’s voice may sound unexpectedly nasal, slurred, or faint. They may also notice a tendency to cough or sputter while drinking thin liquids.
As the condition advances from its subtle beginnings to more widespread neurological changes, the presentation shifts significantly. To understand the evolutionary trajectory of the clinical presentation, review the visual comparison table below.
Symptoms at a Glance: Progression Timeline
| Early Symptoms | Advanced Symptoms |
| Weak grip | Severe muscle wasting (atrophy) |
| Foot drop | Difficulty swallowing (dysphagia) |
| Slurred speech | Respiratory weakness & breathlessness |
| Localized muscle twitching | Widespread loss of physical mobility |
4. When Should You Seek Medical Attention for Possible MND?
You should seek medical attention from a specialized neurologist if you experience persistent, progressive muscle weakness, unexplainable changes in speech clarity, frequent choking, or localized muscle twitching that worsens over several weeks. While these symptoms are often caused by more common conditions, an early, thorough investigation is essential for an accurate diagnosis.
Key Takeaway: Do not ignore localized weakness or changes in speech that develop slowly without a clear physical injury; getting a professional neurological assessment provides clarity and helps exclude treatable conditions.
1. Detailed Explanation
A prompt consultation with an experienced clinical specialist is highly recommended if you or a family member notice certain progressive functional changes. These diagnostic red flags are distinct because they do not resolve with rest and cannot be linked to an acute physical injury:
Progressive, Unilateral Weakness: Noticing that one limb is steadily losing functional power such as repeatedly dropping light objects or dragging a foot while walking indicates an ongoing motor issue.
Changes in Speech and Voice: Gradual onset of slurred speech, a hoarse or nasal tone, or finding it difficult to project your voice during regular conversations.
Swallowing Difficulties: Experiencing an unusual tendency to cough, sputter, or choke when consuming liquids, saliva, or solid food.
Persistent Fasciculations: Frequent, continuous muscle twitching beneath the skin that stays confined to a single muscle group and is accompanied by a measurable loss of strength.
5. Why Does MND Cause Muscle Weakness?
MND causes muscle weakness because the physical muscle tissue is completely starved of the electrical stimulation it requires to contract and function. When the connecting motor neurons die, the muscle fibers become permanently inactive, causing them to lose mass, become rigid, and waste away.
Key Takeaway: Muscles require continuous electrical impulses from nerves to remain healthy and strong; when MND destroys these nerves, the muscles naturally waste away from a lack of use.
1. Detailed Explanation
Muscles are entirely dependent on the nervous system to maintain their structural integrity and tone. Every voluntary physical movement requires an electrical current to travel from the brain, down the spine, and across a microscopic gap to the muscle fibers. This process instructs the muscle tissue to contract.
When Motor Neurone Disease damages these pathways, the electrical connection is severed. Because the muscle tissue is no longer receiving instructions, it falls into a state of permanent disuse. Over time, this lack of stimulation causes the muscle fibers to shrink in volume, a clinical phenomenon known as amyotrophy or muscle wasting. This degeneration also triggers spontaneous, involuntary electrical misfires inside the dying muscle tissue, which patients experience as visible muscle twitching (fasciculations) and painful cramps.
6. What Causes MND?
The exact cause of Motor Neurone Disease remains unknown in the vast majority of cases, but researchers believe it results from a combination of genetic factors and environmental triggers. Approximately 90% of cases occur randomly without any family history, while the remaining 10% are directly inherited through familial genetic mutations.
Key Takeaway: Most cases of MND are sporadic and happen entirely at random, likely driven by an underlying genetic vulnerability combined with environmental stressors.
1. Detailed Explanation
Medical science classifies the causes of motor neurone disease into two distinct categories: sporadic and familial. Understanding these classifications helps specialized medical teams determine the necessary diagnostic and genetic screening approaches.
Sporadic MND (90% of cases): This form develops completely at random in individuals with no prior family history of the disease. While a singular cause has not been isolated, ongoing neurological research suggests it may be triggered by factors like glutamate toxicity (where an accumulation of a chemical messenger damages nerve cells), oxidative stress (cellular damage from unstable molecules), or mitochondrial dysfunction (energy failure within the cell).
Familial MND (10% of cases): This form is directly inherited and runs in families. It is caused by specific, identifiable mutations in certain genes, such as the SOD1, C9orf72, or TARDBP genes. These mutated genes produce faulty proteins that accumulate inside the motor neurons, causing them to fail prematurely.
7. Is MND Hereditary?
Motor Neurone Disease is not hereditary for the vast majority of patients, as roughly 90% of all diagnosed cases are sporadic and occur completely at random. However, for the remaining 10% of individuals who have familial MND, the condition is directly linked to an inherited genetic mutation passed down through generations.
Key Takeaway: Unless you have multiple close relatives diagnosed with the condition, your individual risk of developing MND based purely on family history is exceptionally low.
1. Detailed Explanation
The distinction between sporadic and hereditary neurodegenerative disorders is a common area of patient concern. If an individual develops sporadic MND, their children or siblings do not carry a significantly elevated risk of developing the condition themselves. The disease is simply an isolated event.
Conversely, in familial cases, the genetic mutation is typically passed down in an autosomal dominant pattern. This means that a child of a parent carrying the mutated gene has a 50% chance of inheriting the mutation. In recent years, advanced genetic testing panels have made it possible for an experienced neurologist to identify these specific mutations through a simple blood or saliva sample, providing clear answers for families with a history of neurological disorders.
8. How Is MND Diagnosed?
MND is diagnosed through a careful process of clinical elimination because there is no single test, blood draw, or scan that can instantly confirm the disease. Neurologists use advanced diagnostic tests such as Electromyography (EMG) and MRI scans primarily to rule out other treatable spinal or muscular conditions that mimic MND symptoms.
Key Takeaway: Diagnosing MND relies heavily on Electromyography (EMG) to confirm active nerve damage in the muscles, combined with high-resolution MRI scans to rule out compressed spinal discs or tumors.
1. Detailed Explanation
Because early signs of motor neurone disease like localized muscle twitching or weakness are common to many treatable conditions, a systematic diagnostic approach is essential. A comprehensive neurological evaluation typically includes several specialized investigations:
Detailed Clinical Examination: An experienced neurologist will meticulously assess upper motor neuron reflexes (checking for stiff spasticity and overactive reflexes) and lower motor neuron signs (identifying muscle wasting and fasciculations) presenting across multiple areas of the body.
Electromyography (EMG): Tiny needle electrodes are inserted directly into different muscles to record electrical activity at rest and during use. The EMG can detect subtle, widespread nerve degeneration long before physical muscle wasting becomes visible.
Nerve Conduction Studies (NCS): Small electrical pulses are applied to the skin to measure the speed and strength of your peripheral nerves, helping to ensure the issue isn’t a primary nerve disease like neuropathy.
Magnetic Resonance Imaging (MRI): High-resolution MRI scans of the brain and entire spinal cord are vital to rule out structural mechanical problems, such as a severely herniated cervical disc, spinal stenosis, or spinal tumors, which can compress nerves and mimic MND.
9. Can MND Be Prevented or Cured?
At present, Motor Neurone Disease cannot be cured or entirely prevented, but modern medical management can significantly slow its progression and alleviate symptoms. Current treatments focus on preserving daily physical functioning, reducing discomfort, and supporting respiratory health through advanced therapies.
Key Takeaway: While a definitive cure for MND does not yet exist, evidence-based management plans and specialized pharmacological therapies help protect nerve cells and extend independence.
1. Detailed Explanation
MND remains an irreversible condition because modern medicine cannot currently regenerate dead or severely damaged motor neurons. However, a comprehensive management plan implemented by a multidisciplinary medical team can alter the course of the disease and improve life expectancy.
Pharmacological options include medications like Riluzole, which works by reducing excessive levels of glutamate around the nerve cells, thereby protecting them from chemical toxicity and modestly extending a patient’s survival. Newer treatments, such as Edaravone, function as powerful antioxidants to curb cellular oxidative stress, helping patients preserve their physical mobility for a longer period during the early stages of the condition.
Furthermore, lifestyle modifications, physical therapy to manage joint stiffness, and specialized nutritional protocols play an essential role in preserving comfort and structural stability.
10. How Long Can Someone Live With MND?
Life expectancy with Motor Neurone Disease varies widely based on the specific type diagnosed, but the average survival time is typically between 2 to 5 years from the onset of symptoms. However, some individuals experience a much slower progression of the disease and can live active lives for a decade or longer.
Key Takeaway: Prognosis is highly individualized; while some forms of MND progress rapidly, a significant percentage of patients live well beyond the average timeline with appropriate medical support.
1. Detailed Explanation
A patient’s individual timeline is heavily influenced by the specific motor neuron groups that are damaged first. For example, individuals diagnosed with Primary Lateral Sclerosis (PLS) often experience a very slow, non-fatal progression that allows them to live for decades.
Conversely, when the disease begins with bulbar onset (affecting swallowing and speech) or rapidly targets the respiratory muscles, the timeline tends to move more quickly. Modern supportive interventions such as Non-Invasive Ventilation (NIV) machines that assist the chest muscles at night and specialized feeding tubes (PEG) that prevent malnutrition and accidental choking have proven highly effective at extending survival and maintaining patient comfort.
Specialist Neurological Care at CANES Clinic
Navigating complex neurological changes requires a medical team that combines diagnostic precision with structured, compassionate support. At CANES Cardio & Neuro Clinic, Dr. Soumya Reddy Best Neurologist in Kondapur, we prioritize thorough patient education and evidence-based care paths above all else. We understand that vague physical symptoms can cause significant anxiety, and we are dedicated to providing clear, reliable answers without using alarmist or sensationalized language.
Our facility in Kondapur is equipped with advanced neuro-diagnostic testing options to conduct comprehensive neurological evaluations. Working under a multidisciplinary model, our experienced neurologist ensures that every diagnostic angle is fully explored, systematically ruling out highly treatable conditions that frequently mimic more severe disorders. If you or a loved one are experiencing persistent muscle twitching, sudden weakness in the limbs, or changes in vocal clarity, scheduling a clinical evaluation is a vital step toward protecting your long-term health.
Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Rd, Kondapur, Hyderabad
Contact: +91 9014944654
Appointment Booking: CANES Clinic Official Portal
Key Points to Remember
Core Definition: Motor Neurone Disease is a progressive condition that breaks down the nerve pathways controlling voluntary movement while leaving your senses completely healthy.
ALS Relationship: ALS is simply the most common form of MND, representing a specific variant where upper and lower motor neurons fail together.
Diagnostic Approach: Diagnosis relies heavily on detailed clinical exams, EMG nerve testing, and structural MRI scans to carefully rule out other treatable spinal issues.
Proactive Management: While a cure does not exist, specialized medications, respiratory support devices, and physical therapy significantly extend independence and comfort.
Frequently Asked Questions (FAQs)
A: MND can theoretically present at any stage of adulthood, but it is most frequently diagnosed in individuals between the ages of 50 and 70. Sporadic cases tend to appear slightly later in life, whereas familial variants can sometimes manifest earlier.
A: No, persistent physical numbness, burning, or a “pins-and-needles” sensation are classic symptoms of sensory nerve issues. Because MND targets motor neurons exclusively, these sensory symptoms suggest an alternative diagnosis, such as peripheral neuropathy or a pinched nerve disc.
A: Yes, isolated muscle twitching (fasciculation) is an incredibly common condition that is frequently triggered by high stress, lack of sleep, excessive caffeine intake, or minor electrolyte imbalances. It is rarely a sign of MND unless it occurs alongside progressive, objective muscle weakness or wasting.
A: A mini-stroke (Transient Ischemic Attack) causes a sudden, immediate loss of neurological or muscular function due to a temporary lack of blood flow to the brain, and symptoms typically resolve within hours. MND, by contrast, is a slow, gradual, and steadily progressive degeneration of nerve cells over months and years.
A: Yes, the vast majority of individuals with MND retain their complete cognitive abilities, memory, and reasoning skills. While a small percentage of patients may experience mild cognitive or behavioral shifts, the core intellectual faculties of the brain generally remain entirely uncompromised.
A: When bulbar muscles weaken, swallowing food and liquids becomes difficult and physically dangerous, as debris can accidentally enter the lungs (aspiration). A specialized feeding tube ensures the patient receives safe, balanced hydration and nutrition directly into the stomach without the risk of choking.
Expert Care
Hyderabad's leading Cardio & Neuro specialists.
