What Is Motor Neurone Disease? Understanding the Causes, Symptoms, Diagnosis, and Treatment
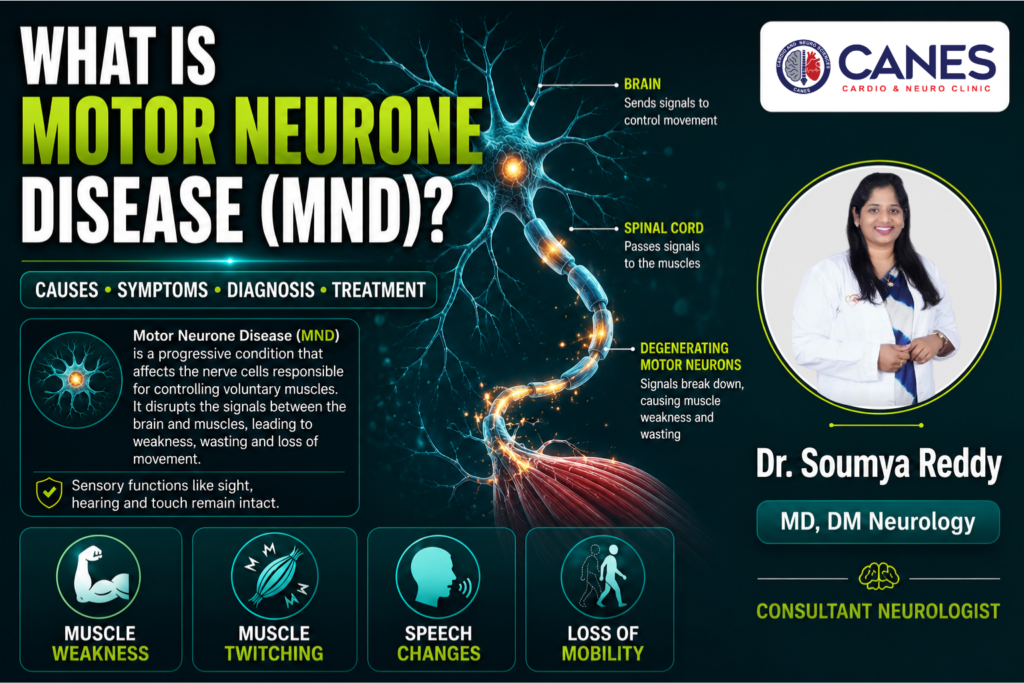
● Lifestyle & Prevention What Is Motor Neurone Disease? Understanding the Causes, Symptoms, Diagnosis, and Treatment Table of Contents Introduction 1. What Is Motor Neurone Disease? 2. Is MND the Same as ALS? 3. What Are the First Signs of MND? 4. When Should You Seek Medical Attention for Possible MND? 5. Why Does MND Cause Muscle Weakness? 6. What Causes MND? 7. Is MND Hereditary? 8. How Is MND Diagnosed? 9. Can MND Be Prevented or Cured? 10. How Long Can Someone Live With MND? FAQs Book a Consultation Prevention is better than cure. Talk to our specialists today. Book Now Experiencing unexplained muscle weakness, muscle twitching, or subtle changes in speech can be deeply concerning. The human nervous system relies on a continuous, uninterrupted exchange of electrical signals to coordinate everyday actions. When these communication pathways begin to degrade, simple tasks like gripping an object or walking on a flat surface can become increasingly difficult. Securing a comprehensive evaluation from a medical professional is the most critical step in identifying the root cause of these neurological changes and establishing an evidence-based management plan. Quick Answer : Motor Neurone Disease (MND) is a progressive neurodegenerative disorder that systematically destroys the nerve cells responsible for voluntary muscle movement. The condition interrupts the electrical signals between the brain and muscles, leading to muscle wasting, weakness, loss of mobility, and eventual respiratory challenges. While there is currently no cure, advanced diagnostics and multidisciplinary care significantly improve symptom management and quality of life. 1. What Is Motor Neurone Disease? Motor Neurone Disease (MND) is a group of progressive neurological disorders that selectively destroy motor neurons, the specialized nerve cells controlling voluntary muscle movements. As these neurons degenerate, the brain loses its ability to communicate with muscles, resulting in muscle weakness, wasting (atrophy), and difficulties with speaking, swallowing, and breathing. Key Takeaway: Motor Neurone Disease targets the nerve cells that control voluntary movement, cutting off communication between the brain and the muscular system, while leaving sensory functions like sight and touch intact. 1. Detailed Explanation To understand this neurodegenerative disorder, it helps to examine the anatomy of the nervous system. Voluntary movements such as walking, lifting objects, and talking require a two-part nerve pathway: Upper Motor Neurons: These cells are located in the brain and send electrical instructions down through the spinal cord. Lower Motor Neurons: These cells accept the signals in the spinal cord and extend outward to directly stimulate muscle tissue. In an individual with Motor Neurone Disease, both upper and lower motor neurons gradually break down and die. When these cells degenerate, the vital electrical messages can no longer span the anatomical gap. Starved of stimulation, the muscles begin to weaken and naturally shrink over time. Crucially, because MND specifically attacks motor pathways, the sensory nervous system remains fully functional; a patient’s ability to see, hear, smell, taste, and feel physical touch on the skin is entirely preserved. 2. Is MND the Same as ALS? Amyotrophic Lateral Sclerosis (ALS) is the most common and widespread form of Motor Neurone Disease, but it is not the only type. While the terms are often used interchangeably in casual conversation or general media, MND is the broader umbrella medical classification that includes several other distinct neurological variants. Key Takeaway: ALS is a specific type of Motor Neurone Disease that damages both upper and lower motor neurons, representing the vast majority of all global MND diagnoses. 1. Detailed Explanation In medical terms, Motor Neurone Disease acts as a category heading. Amyotrophic Lateral Sclerosis accounts for approximately 85% to 90% of all cases within this category. In ALS, the degeneration occurs simultaneously in both the upper motor neurons of the brain and the lower motor neurons of the spinal cord, leading to widespread physical weakness that affects the limbs, speech, and respiratory system. However, other variants exist depending on which specific parts of the motor pathway are affected. To understand the different types of conditions that fall under the MND umbrella, review the clinical comparison table below: MND Classifications: ALS vs. PLS vs. PMA vs. PBP Feature Amyotrophic Lateral Sclerosis (ALS) Primary Lateral Sclerosis (PLS) Progressive Muscular Atrophy (PMA) Progressive Bulbar Palsy (PBP) Neurons Affected Both Upper and Lower Upper Motor Neurons only Lower Motor Neurons only Brainstem Bulbar Neurons Primary Symptoms Muscle weakness, wasting, and stiffness Extreme muscle stiffness, slow movement, spasticity Muscle wasting, weakness, and deep twitching Difficulty speaking, slurred speech, choking Onset Location Usually limbs (arms or legs) Usually begins in both legs Usually begins in hands or feet Muscles of the throat and tongue Progression Rate Rapid to moderate Slow, non-fatal variant Slower progression than ALS Rapid, affects breathing early 3. What Are the First Signs of MND? The first signs of Motor Neurone Disease typically manifest as mild, painless, and asymmetrical muscle weakness, such as an unstable hand grip, frequent tripping, or slurred speech. Because these initial physical changes develop gradually, they are frequently mistaken for minor nerve compressions, fatigue, or normal signs of aging. Key Takeaway: Early signs of MND are usually subtle and localized, often presenting as a weak grip in one hand, foot drop in one leg, or minor changes in vocal clarity. 1. Detailed Explanation Because the early signs of motor neurone disease are painless and isolated, many individuals do not immediately recognize the need for a neurological assessment. Clinical observation shows that symptoms usually begin in one of three distinct anatomical regions: The Arms (Limb Onset): Patients may notice an unexpected weakness in their dominant hand. Everyday fine motor tasks, such as fastening buttons, turning keys, opening jars, or writing legibly, become increasingly challenging. The Legs (Limb Onset): Weakness often presents as “foot drop,” where the muscles responsible for lifting the front of the foot weaken. This causes the toes to drag on the ground, leading to unexplainable stumbling or tripping over completely flat surfaces. The Throat and Mouth (Bulbar Onset): The muscles controlling speech and swallowing are affected first. A patient’s voice may sound
